Definition of Cushing Syndrome:
It is a clinical condition in which free circulating glucocorticoids level is increased. Most common cause is iatrogenic due to prolonged administration of synthetic glucocorticoid such as prednisolone.
Classification and Causes of Cushing Syndrome:
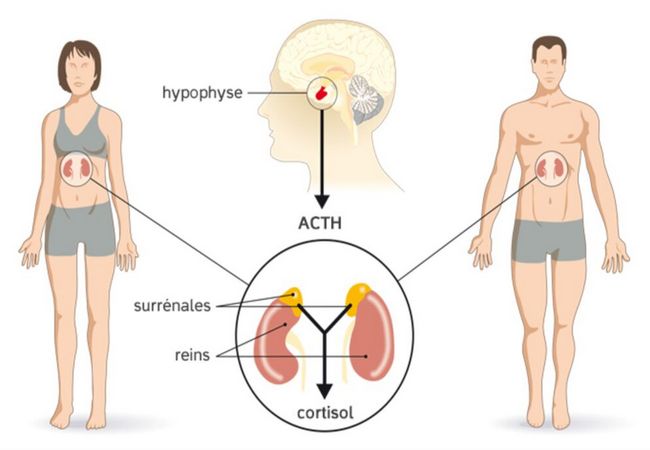
1. ACTH dependent:
- Pituitary adenoma secreting ACTH (e.g. Cushing’s disease),
- Ectopic ACTH syndrome (e.g. bronchial carcinoid, small cell lung carcinoma, pancreatic -endocrine carcinoma).
- Iatrogenic (ACTH therapy).
2. Non-ACTH dependent:
- Latrogenic (chronic glucocorticoid therapy, e.g. For asthma),
- Adrenal adenoma,
- Adrenal carcinoma.
3. Pseudo-Cushing’s syndrome : (i.e. cortisol excess as a part of another illness):
- Alcohol excess,
- Major depressive illness,
- Primary obesity.
Clinical Features or Sign and Symptoms of Cushing Syndrome:
1. General appearance:
- Moon face (due to deposition of fat in the face),
- Buffalo neck (due to deposition of fat in the subscapular region),
- Hair thining,
- Hirsutism,
- Acne ,
- Mild exophthalmos,
- Cataract,
- Plethora.
2. Skin:
- Bruising,
- Striae,
- Decreased skin thickness.
3. Musculoskeletal system:
- Wasting & weakness of proximal thigh muscle.
- Loss of height and back pain from compression fracture.
- May have exuberant callus with fractures
- Osteoporosis
4. Abdominal:
- Centripedal obesity or Pendulous abdomen (due to deposition of fat in the abdomen & buttock,
- Peptic ulcer.
5. Tendency to infections with poor wound healing and little inflammatory response
6. Hypertension
7. Genitourinary:
- In male- impotence (due to atrophy of testes)
- In female- amenorrhoea (due to atrophy of ovary)
8. Hyperglycaemia
9. Psychosis.
Investigation of Cushing Syndrome:
To confirm the Dx:
- 24 Urinary free cortisol level – raised.
- Overnight dexamethasone suppression test: Fail to suppress.
- Diurnal rhythm of plasma cortisol: evening level >75% of morning level in Cushing’s.
To detect the cause:
- Plasma ACTH level.
- Excess cortisol + undetectable ACTH- Adrenal tumor.
- Detectable ACTH-Pituitary adenoma secreting ACTH (e.g. Cushing’s disease) or Ectopic ACTH syndrome.
- Plasma CRH test & High dose dexamethasone suppression test
- Adrenal USG, CT scan or MRI.
- MRI for Cushing’s disease.
- Inferior petrosal sinus sampling for Cushing’s disease (>200% of ACTH conc.)
Treatment of Cushing Syndrome:
1. Medical therapy: Metyrapone, Ketoconazole- inhibit cortisol synthesis.
2. Cushing’s disease:
- Trans-sphenoidal surgical removal of pituitary adenoma.
- If no tumor is found & Dx is Cushing’s disease – radical hypophysectomy may be required.
- Bilateral adrenalectomy with pituitary irradiation to prevent Nelson’s syndrome.
3. Adrenal tumors:
- Adenoma: Removed via laparoscopy or loin incision.
- Carcinoma: Resected if possible or Irradiation & adrenolytic drug is given to the pt.
4. Ectopic ACTH syndrome:
- Bronchial carcinoid is removed.
- Malignancies – Radiotherapy, chemotherapy according to choice.
5. Iatrogenic Cushing’s syndrome:
- Gradually tapering the receiving steroid & ultimately stop if possible.
How Will You Differentiate Cushing’s Syndrome from Myxedema Clinically?
Points of Difference | Myxedema | Cushing’s Syndrome |
Voice | Hoarseness of voice | Normal voice |
Reaction to hot | Cold intolerance | Not such |
Thyroid swelling | Goitre usually present | Not present |
Appearance | Puffy face with baggy | Moon face with |
Weight gain | Periorbital oedema | Central obesity is |
Easy bruising | Not present | Present |
Skin condition | Increased thickness | Decreased skin |

Maria Khatun Mona is a Founder and Editor of Nursing Exercise Blog. She is a Nursing and Midwifery Expert. Currently she is working as a Registered Nurse at Evercare Hospital, Dhaka, Bangladesh. She has great passion in writing different articles on Nursing and Midwifery. Mail her at “maria.mona023@gmail.com”